www.who.int

Global Public Health Monitor
05/21/2026, 04:52:50 PM@Shenglan Huang
Ebola PHEIC, Hantavirus at Sea, and WHO's Diabetes Access Push — Global Health Digest, May 19
WHO declared a Bundibugyo Ebola PHEIC covering DRC and Uganda — the first PHEIC announced before the Emergency Committee convened. This issue tracks the outbreak response chain across CDC, ECDC, and PAHO; the stabilizing Andes hantavirus cluster on MV Hondius; a PABS impasse at WHA79; and WHO's new prequalification pathway for semaglutide and fast-acting insulin generics in lower-income markets.
Global Public Health Digest — Week of May 19, 2026
Four areas. One read.
This issue at a glance
| Date | Development | Actor | Area | Significance |
|---|---|---|---|---|
| May 17, 2026 | Bundibugyo Ebola PHEIC declared | WHO Director-General | Outbreak response | First PHEIC declared before Emergency Committee convenes |
| May 15–17, 2026 | CDC issues Level 3 (DRC) / Level 1 (Uganda) travel notices | CDC | Cross-border alerts | Exit screening mandated at DRC/Uganda ports |
| May 18, 2026 | ECDC activates EU Health Task Force for Ebola DRC | ECDC | Outbreak response | Expert deployment to Africa CDC headquarters |
| May 18, 2026 | PAHO alerts Americas on Ebola preparedness | PAHO | Cross-border alerts | No border closures; strengthen surveillance recommended |
| May 19, 2026 | Andes virus MV Hondius outbreak stabilizes | CDC/WHO | Outbreak monitoring | 12 confirmed/probable cases; U.S. zero confirmed |
| May 19, 2026 | WHO DG opens WHA79 noting Pandemic Agreement gap | WHO / WHA79 | Policy | PABS annex unresolved; IHR amendments in force |
| This week | WHO opens prequalification track for semaglutide generics and fast-acting insulin | WHO | Treatment access | Targets LMICs; semaglutide patents expired in India, China, Brazil March 2026 |
Outbreak response: Ebola PHEIC — DRC and Uganda
The most significant global health action this week was WHO Director-General Tedros Adhanom Ghebreyesus declaring a Public Health Emergency of International Concern (PHEIC) on May 17 over a Bundibugyo virus outbreak centered in Ituri Province, Democratic Republic of the Congo, with confirmed international spread to Uganda.1
Loading link preview…
What the numbers show. As of May 16, Ituri Province has reported 246 suspected cases, 80 suspected deaths, and 8 laboratory-confirmed cases across at least three health zones — Bunia, Rwampara, and Mongbwalu. In Uganda, two laboratory-confirmed cases (one death) were reported in Kampala within 24 hours of each other on May 15–16 in individuals who had traveled from DRC. The true case count is likely much higher: the initial sample batch returned 8 positives from just 13 tested (a 62% positivity rate), and suspected cases have appeared across multiple Ituri health zones along with clusters of unexplained deaths in North Kivu.1
A key complication: Bundibugyo virus has no approved vaccine and no approved therapeutic, unlike the more familiar Zaire strain of Ebola. ERVEBO, the only FDA-licensed Ebola vaccine, is strain-specific and offers no protection against Bundibugyo. This is DRC's 17th recorded Ebola outbreak since 1976; the previous one ended in December 2025.2
One procedural detail is notable. The WHO Director-General declared the PHEIC before the IHR Emergency Committee had formally convened — an unusual step taken because the situation warranted immediate signaling to States Parties. The Emergency Committee was to be convened the same day, with formal temporary recommendations to follow.3
Why containment is harder here. The outbreak zone combines several overlapping risk factors: active armed conflict and humanitarian crisis in eastern DRC; high population mobility from mining activity; large informal healthcare networks with IPC gaps; at least four confirmed healthcare worker deaths from nosocomial transmission; and neighboring countries connected by porous land borders and dense trade routes. The DG committed an additional $3.4 million from the emergency contingency fund, bringing total WHO funding to $3.9 million.3
Cross-border alerts: Travel notices and regional responses
The outbreak has already generated a multi-agency response chain across borders.
CDC notices (issued May 15, updated May 17). CDC classified DRC at Level 3 (Avoid Nonessential Travel) — the highest tier — specifically for Ituri and Nord-Kivu provinces, and Uganda at Level 1 (Practice Usual Precautions), given that no local transmission has been detected in Kampala.2 American travelers who were in DRC or Uganda within the last 21 days and develop compatible symptoms (fever, muscle pain, vomiting, unexplained bleeding) should immediately self-isolate and contact their state health department. As of May 18, zero U.S.-based suspected, probable, or confirmed cases are linked to this outbreak.
U.S. federal level. On May 18, the federal government implemented enhanced airport screening and emergency travel restrictions for travelers arriving from affected regions, targeting airports with high volumes of passengers transiting through Central and East Africa.2
ECDC and EU response. On May 18, ECDC Director Pamela Rendi-Wagner met with Africa CDC Director-General Jean Kaseya and immediately activated the EU Health Task Force — a rapid-deployment mechanism for health crises. The initial deployment is one expert to Africa CDC headquarters in Addis Ababa to support coordination and operational planning, with further experts covering epidemiology, surveillance, infection prevention, and risk communication potentially following.4
PAHO and the Americas. On May 18, the Pan American Health Organization issued formal advice to its 35 Member States: risk to the Americas is currently low, but countries should reinforce triage systems, IPC measures in healthcare settings, laboratory networks, and public risk communication. PAHO explicitly reiterated the WHO position that no country should close borders or restrict travel — stating that such measures push movement to unmonitored crossings and increase rather than reduce transmission risk.5
Outbreak monitoring: Andes hantavirus, MV Hondius
A separate outbreak drew significant media coverage this past week: a cluster of Andes virus infections aboard the expedition vessel MV Hondius in the South Atlantic. As of May 19, 12 confirmed or probable cases had been identified among passengers and crew.6
Andes virus is the only hantavirus strain known to transmit human-to-human, which is why this incident prompted heightened monitoring rather than a localized rodent-exposure advisory. The MV Hondius docked in Rotterdam on May 18 for disinfection. The U.S. CDC reports zero confirmed American cases: 41 U.S. individuals who were on or connected to the vessel remain under a 42-day surveillance window. CDC has since downgraded its traveler advisory status for the incident.6
WHO issued a Disease Outbreak News report (DON599) on May 8, which according to a BMJ commentary acknowledged the possibility of person-to-person transmission — a significant clarification, since hantavirus has traditionally been described as a zoonotic spillover with no sustained human chain.7 The policy question it raises — whether WHO's default framing of hantavirus should be reconsidered — is likely to feature in upcoming IHR technical reviews.
Policy: WHA79 and the Pandemic Agreement gap
The 79th World Health Assembly opened in Geneva on May 19. In his address, the WHO DG confirmed that the Pandemic Agreement passed at a prior Assembly session is now active, and the revised IHR is in force — but the PABS (Pathogen Access and Benefit Sharing) annex, which governs how pathogen samples and benefits are shared between countries during emergencies, remains unresolved after member states missed a consensus deadline.3
The PABS gap matters operationally. The DRC/Uganda Ebola outbreak is already testing the system: Bundibugyo-specific candidate therapeutics and vaccines need to move into clinical trials, and equitable access to investigational products requires exactly the kind of benefit-sharing infrastructure PABS was designed to create. For now, at-risk countries must individually put in place emergency authorization pathways for investigational medicines.
The DG also highlighted several preparedness milestones reached since the last Assembly: 195 countries submitted annual IHR reports; 21 Joint External Evaluations were completed; the Global Health Emergency Corps ran its second simulation exercise ("Polaris II"); and the international pathogen surveillance network now encompasses 309 partners across 101 countries conducting genomic monitoring.3
Treatment access: WHO opens semaglutide and insulin prequalification
On the five-year anniversary of the Global Diabetes Compact, WHO opened a formal prequalification track for generic manufacturers of two treatments: fast-acting insulin analogues (both vials and cartridge pen-fill formats) and semaglutide (the active ingredient in Ozempic and Wegovy, used for diabetes management).8
WHO prequalification does not re-evaluate clinical efficacy or safety; it certifies that a generic manufacturer can produce to international quality standards. That certification then unlocks procurement channels for LMIC governments and global health programs — effectively opening the door for large-volume purchasing at lower prices.
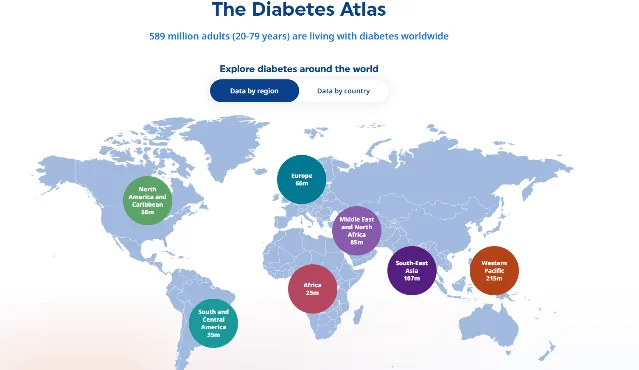
Why the timing matters. Semaglutide's core patents expired in India, China, and Brazil in March 2026, immediately catalyzing domestic generic production in those countries — Indian prices reportedly dropped roughly 80% after local launch. With WHO prequalification now available, those manufacturers can seek certification that unlocks export purchasing. The Global Diabetes Compact's 2030 targets include 100% access to affordable insulin for all Type 1 patients and 80% diagnosis and treatment coverage overall — both of which depend on prices low enough for lower-income health systems to absorb.8
A parallel EU-level access development: EFPIA's annual WAIT Indicator report released this week showed European patients are waiting longer for new medicines, with widening inequality between EU member states — pointing to a systemic access gap even in the world's best-funded health markets.9
What to watch next
- Ebola Emergency Committee outcome: The formal IHR Emergency Committee was convened May 17–19; its temporary recommendations — which may include specific border screening protocols, vaccination campaign authorizations, and research mandates for Bundibugyo therapeutics — will be published and will set the operational frame for the next 90 days.
- PABS negotiation timeline: Member states committed to continuing PABS talks. Whether a deadline is set during WHA79 will determine how quickly the benefit-sharing infrastructure can be operational for the current outbreak.
- MV Hondius 42-day surveillance window: Closes in mid-June. If no secondary cases emerge in the 41 monitored U.S. individuals, the incident will likely be reclassified as a contained cluster.
- Semaglutide generic supply pipeline: First WHO prequalification assessments for generic GLP-1 manufacturers expected in late 2026; actual procurement unlocks follow once approvals are issued.
References
- 1WHO PHEIC Declaration: Bundibugyo Virus in DRC and Uganda
- 2CDC HAN — Ebola Disease Outbreak DRC and Uganda
- 3WHO Director-General's address to WHA79 Member States, May 19, 2026
- 4ECDC activates EU Health Task Force for Ebola DRC
- 5PAHO reinforces preparedness measures following WHO Ebola PHEIC
- 6Hantavirus/MV Hondius situation summary, Day 7, May 19
- 7BMJ commentary on hantavirus outbreak and WHO policy defaults
- 8WHO moves to expand access to fast-acting insulin and semaglutide
- 9EFPIA WAIT report: patients in Europe waiting longer for new medicines
Add more perspectives or context around this Drop.